Dentures That Feel Natural, Look Beautiful.
Impacted Wisdom Tooth: Causes, Jaw Lock Symptoms, Healing Timeline, and Safe Salt Water Rinse Routine
Image:

Severity:
Teeth Problems:
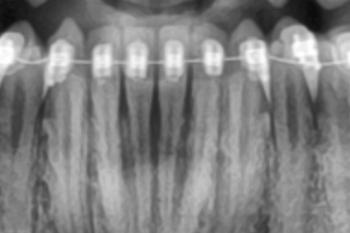
Quick radiographic findings (what I see)
-
Impacted mandibular third molar(s) (wisdom tooth/teeth) with a mesio-horizontal / mesioangular impaction — the crown is tipped toward the second molar and is at least partially covered by bone/soft tissue.
-
The impacted crown is in close proximity to the distal surface/roots of the adjacent second molar → this raises risk of decay/resorption of the second molar and increased surgical difficulty.
-
The roots of the impacted tooth appear to be close to the mandibular canal (inferior alveolar nerve) on the panoramic film — panoramic images can underestimate proximity; a CBCT (cone beam CT) is recommended to assess true nerve relationship.
-
No obvious large cyst or gross bone destruction visible on this single panoramic image, but panoramic films are limited for fine detail.
Most likely clinical problems from this x-ray
-
Recurrent pericoronitis (infection around the partially erupted tooth)
-
Caries on the impacted tooth or on the distal of the second molar due to food trapping
-
Periodontal bone loss distal to second molar
-
Increased difficulty with extraction and higher risk of temporary/permanent inferior alveolar nerve (IAN) disturbance if roots are very close to the canal
Does this make your jaw “locked”?
-
The radiograph suggests an impacted wisdom tooth that can cause trismus (reduced ability to open) if there is significant infection, inflammation, or muscle spasm.
-
“Locked jaw” (true lockjaw / tetanus is rare) — more commonly after impacted wisdom problems patients experience trismus: pain and reduced mouth opening.
-
If you are currently unable to open your mouth at all, or with severe pain, or if you have fever/swelling, seek urgent dental care.
Salt (saline) rinses — is it OK to do long term?
-
Short term (post-op / during healing): warm saline rinses (1/2–1 tsp salt in 250 mL warm water) 3× daily are excellent and recommended once you can rinse (typically after 24 hours post-extraction). Good for 7–14 days to promote healing and reduce bacteria.
-
Long term (weeks to months): occasional saline rinses are safe and non-harmful, but doing them every day for many months is usually unnecessary. If you have chronic irritation or a persistent open wound, daily saline is reasonable while you see a dentist.
-
Caveat: saline will not treat an ongoing infection that requires antibiotics or surgery. If symptoms persist despite rinses, get definitive treatment.
Recommended next diagnostic step
-
CBCT (cone-beam CT) of the area to precisely evaluate the relation of the tooth roots to the inferior alveolar nerve and the exact angulation — this changes the surgical plan and consent regarding nerve risk.
Typical extraction workflow (what to expect)
-
Pre-op visit: medical history, consent, pano + possibly CBCT, discuss anesthesia options (local ± sedation or general).
-
Pre-op instructions: fasting if sedation/GA, stop/adjust anticoagulants only as directed by physician/dentist.
-
Day of surgery: local anesthesia ± IV sedation / GA. For deeply impacted teeth the surgeon will raise a flap, remove bone around tooth, section the tooth if necessary, remove roots, irrigate, suture.
-
Immediate post-op: pressure control, pain control, cold packs first 24–48 hrs, then warm compresses; soft diet; avoid smoking/straws; follow meds (analgesics ± antibiotics if indicated).
-
Follow-up: 3–7 days to check healing and remove sutures if non-resorbable; re-evaluate at 2 weeks and later if needed.
Typical healing timeline (if uncomplicated)
-
0–48 hours: peak pain and swelling; bleeding should be controlled.
-
3–5 days: swelling and pain typically start to subside. Continue soft diet.
-
7–10 days: sutures may be removed (if applicable). Significant reduction of pain and swelling.
-
10–14 days: soft tissue mostly healed; you should be improving daily.
-
4–6 weeks: soft tissue and comfort usually good, though bone remodeling continues.
-
6–12 months: bone remodeling and complete radiographic healing.
If at 14 days you still have severe pain, swelling, pus, persistent heavy bleeding, or numbness — return to your surgeon/dentist immediately.
Possible complications (what could scale up if untreated / or after extraction)
-
If extraction delayed/left untreated: recurrent infection (pericoronitis), spread of infection to deep spaces (submandibular, parapharyngeal) → can be serious, difficulty swallowing or breathing. Progressive decay of adjacent tooth or periodontal destruction. Cyst formation around impacted tooth (dentigerous cyst).
-
After extraction risks: dry socket (alveolar osteitis) — severe pain around day 3–5, requires treatment; infection — needs antibiotics & drainage; inferior alveolar nerve injury — numbness/tingling of lower lip/chin (usually temporary, rarely permanent); lingual nerve involvement (taste/sensation) possible; bleeding; trismus; very rarely jaw fracture or osteomyelitis in compromised patients.
-
Early recognition is key — persistent or worsening symptoms should be seen urgently.
Immediate advice / steps you can take now
-
If you have significant opening limitation, fever, progressive swelling, increasing pain, pus, difficulty breathing or swallowing → seek emergency dental care now.
-
Continue gentle warm saline rinses (3× daily) — fine for now. If extraction is planned, follow your surgeon’s instructions (they may ask you to stop rinsing before/after surgery or use for a limited time).
-
Maintain excellent oral hygiene around the area but avoid aggressive probing of the inflamed tissue.
-
Avoid smoking and alcohol (they impair healing).
-
Arrange CBCT evaluation if your surgeon recommends it.
-
Book extraction with an oral surgeon if you decide on removal; discuss anesthesia type and nerve-risk based on CBCT.
What to tell your dentist/surgeon (sample points to bring up)
-
Show this x-ray and ask if they recommend CBCT and why.
-
Ask about IAN proximity and the chance of temporary vs permanent numbness (percent based on their assessment).
-
Ask whether to expect a simple or surgical extraction, anesthesia options, antibiotic plan, and estimated recovery timeline.
-
If cost or time is a concern, ask about staged care (treat infection first, then extraction).
Visit nearest clinic / directory
-
You included your clinic directory link — bring the x-ray file and your symptoms history (duration, fever, swelling, mouth opening, prior infections) when you visit. If you want, I can help you write a short message to send to the clinic describing symptoms and requesting an appointment.
If you want, I can:
-
Draft a clear message you can send to the clinic/dentist including the key concerns (jaw locking/trismus, duration, rinses).
-
Create a short checklist of questions to ask your surgeon before extraction.
-
Explain post-op care day-by-day in printable format.
Tell me which of those you want and I’ll prepare it right away.
Related Clinical Cases
Patients with lower front gum inflammation may also experience tartar buildup, periodontal disease, gum abscesses, or tooth decay. Explore these related clinical case studies.